

Our operations for pilonidal cyst
The experience of over 20 years of surgery flows into the surgical treatment of our patients.
The minimally invasive therapy is always preferred by us.
There are various options for the treatment of pilonidal cyst (pilonidal sinus). The common factor is that so far only surgical therapy is available as a cure. Conservative therapy, even with the administration of antibiotics, is not possible. The surgical method depends very much on the severity of the findings.
Acute inflammation
This condition usually occurs with a collection of pus (abscess) and immediate surgical repair is required. An abscess is always an emergency indication. Smaller abscesses of up to 5 cm can usually be opened well on an outpatient basis under local anesthesia.
It is important to cut out some of the skin to ensure good drainage. Only a small incision under icing is not sufficient. Larger abscesses should be operated on in the hospital under general anesthesia, especially if they are located near the anus.
This often results in very large defects that heal slowly over 3-6 months. This is a great physical and psychological burden for the mostly young patients.
Small fistula tracts without inflammation
Here you can see the openings where hairs grow into the depth. These so-called pits can be operated on in a small, painless operation, the pit picking well outpatient. Small wound defects remain that cause little pain and usually heal within 7-14 days. This procedure is purely outpatient, so no hospitalization is necessary.
Large fistula tracts without inflammation:
In these findings, the pit picking procedure reaches its limits, as there are cavities and scars at the end of the canals that have to be excised. A combination here would be pit picking with sinusectomy, in which the scars and the scar cavity are removed with several small incisions.
In the case of recurrent pilonidal cyst without acute inflammation, plastic surgery according to Karydakis, for example, can be performed. In this case, the skin and the subcutaneous fatty tissue are completely removed and followed by a plastic surgery with shifting of the midline to the side in order to close the defect. The wound can be completely sutured closed in the process. This operation is always inpatient.
Overview of open operations

Pit Picking
In classic pit picking, a punch is used to remove the small holes in the center line. The diameter of the wounds is 3-4mm.
For this purpose, a lateral relief cut is made.

Sinusectomy
In the case of larger fistulas, these must also be removed, adding another wound to the defects during pit picking in order to excise the fistula in a tunneled fashion.
Lasertherapy
Here, too, the pits are removed and the laser is inserted over the lateral fistula opening. This procedure is particularly suitable for long, narrow fistula courses.

Excision
Excision. Classic and radical surgery. Often described as the "butcher's method" by patients, as a large hole is created, with a long wound healing time.
Pit Picking
During pit picking, small hair channels are removed from the skin with a punch. These are believed to be the entry points for hairs into the subcutaneous fatty tissue, leading to the dreaded chronic inflammation. Therefore, the complete removal of these hairs is also part of the surgery, otherwise the inflammation will reappear, which is called a recurrence. There must be a lot of experience on the part of the surgeon and the procedure must be performed very thoroughly. The diameter of the punch is 3-4mm.
However, pit picking always includes removal of the abscess cavity present under the pits, where the hair has been deposited. The cavity together with the wall and the hairs must always be removed as well in order to prevent the recurrence of the disease. In this case, the surgical access is always somewhat lateral in order to leave the smallest possible wound in the midline, which heals poorly.
After the operation, the very small wounds remain open to allow the wound secretion that forms to drain away, allowing the wound to clean itself. There is also the possibility of suture closure, but since there is always the residual risk of renewed inflammation with pus formation and the wounds close within 1-2 weeks without a suture, we prefer open wound healing as a safe option.
It is important to know that the disease can recur and the risk of this is about 20-25%. Unfortunately, the classic generous excision of the lesion is still the "gold standard" in surgery of the pilonidal sinus, as there are fewer recurrences, but it leads to a very long wound treatment.
Therefore, pit picking should always be considered as a therapeutic option if the findings are suitable.
Details about Pit Picking

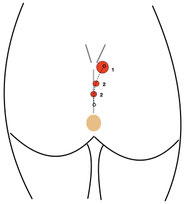
Surgery situs
This figure shows the dimensions of the operation. The center line shows the small pits (1). These are removed with the punch. To clean the underlying cavity, a lateral incision (2) is made and over this the cavity is carefully cleaned of cell debris and irrigated.
After 2-4 weeks, the wound is usually healed.

Punch
This is a typical skin punch with which the pit picking operation is performed under local anesthesia.
The opening is 3-4mm in diameter and the channels are punched out as a whole, which is painless.
The wound secretion drains through the created channel, which cleans the wound from the inside.

After surgery
Wounds after surgery are shown here. Since these are always potentially infectious wounds, they heal openly.
Operation time: 10-15 minutes
Hospitalization: no, outpatient surgery.
Inability to work: approx. 1-5 days
General anesthesia: no, local anesthesia
Sinusectomy
In more extensive findings, a lateral fistula outlet is found above the pits in the midline. Between this fistula outlet and the pits, a rough induration can often be palpated, which corresponds to the 2-5cm long fistula in the subcutaneous fat tissue.
This fistula structure must be completely removed, which we call sinusectomy.
During the operation under local anesthesia, the fistula is cut out via the lateral exit (ectomy) after punching out the pits, without opening the overlying skin. This creates a tunnel, so to speak. Importantly, all diseased tissue must be removed to prevent recurrence.
After the procedure, the small wounds remain open so that the secretion that forms can drain away, allowing the wound to clean itself. The larger wound takes about 3-4 weeks to close.
Details about sinusectomy for pilonidal cyst (sinus pilonidalis)

Sinusectomy
Here, the pits (1) are first punched out and then the fistula (3) is cut out via the fistula outlet (2). The entire cavity (3) with the scar and fistula tissue, which often contains the hair, must be removed.

Postoperative result
Eight weeks after sinusectomy, the wounds have healed completely. The center shows the overgrown pits and the lower left the scar of the fistula outlet, which has also healed without complications.

Fistula in cross section
Operation time: 15-30 minutes
Hospitalization: no, outpatient surgery.
Inability to work: approx. 5-14 days
General anesthesia: no, local anesthesia
Lasertherapy
SiLaC® is a safe procedure to treat coccygeal fistulas. Here, the coccygeal fistula is irradiated with a laser beam using a minimally invasive technique. Minimally invasive here means that only a small operation with minimal wounds is necessary. SiLaC means "Sinus Laser ablation of the cystic duct".
The operations are performed under general anesthesia. During the treatment, which takes only a few minutes, a probe is inserted into the inflamed fistula tract. Laser energy is used to precisely obliterate the fistula tissue without damaging or even removing surrounding tissue. Any incisions made to relieve the abscess are significantly smaller.
As the probe is withdrawn, the fistula tissue is slowly and safely destroyed. The existing cavity collapses and eventually scars over. The extremely flexible probe is well suited for use even in slightly tortuous passages and can therefore be used anywhere.
The small wounds are healed quickly and there is very little secretion of wound fluid in contrast to conventional surgical procedures, where an open wound area remains for several months. There is often swelling in the area of the cavity, which resolves after several weeks and is not painful. Our patients require very little to no pain medication.
Advantages of the laser compared to conventional surgery

- Closure of the fistula tract
- Very low pain
- Minimal wound area
- Excellent healing results
- Clearing out of excess, inflamed tissue as well as residual hair
- Outpatient surgery
- Short treatment time
- Fast recovery
- Only a few days of inability to work - ideal for self-employed people
Operation time: 10-15 minutes
Hospital stay: no, outpatient service
Inability to work: approx. 1 week
General anesthesia: yes
Outpatient surgery: yes
Costs of laser therapy are now covered by many insurance companies!
Since 01.06.2021, the costs for minimally invasive laser therapy have been covered in full by many company health insurances as part of integrated care. Patients from other states in Germany can also undergo minimally invasive surgery with us in Berlin. Please contact us to find out whether your BKK is included.
What is the procedure of laser surgery for pilonidal cyst?

Fistula course
The pit (arrow) is shown on the left. This pit is always located in the midline of the gluteal fold (rima ani) and is usually not painful.
The outlet of the fistula lies above it and is marked here with 2 arrows. In between lies the abscess cavity (black line), which is the actual target of the laser operation and collapses due to the circular heat radiation.

Wound cleansing
First, the fistula tract is exposed with a probe and thoroughly cleaned. The hair in the cavity and dead tissue are removed.
The hairs cause the chronic inflammation. This is followed by extensive irrigation with a disinfecting solution.

Punching
Then the punching out of the existing pits (here only one) is done with a special punch. The diameter is 3-4mm and results in a clean wound edge that can heal well.
The fistula channel is thereby completely removed

Laser treatment
Introduction of the laser diode into the fistula tract and cavity. Closure of the cavity and the duct by multiple, slow retraction.
After the first pass, the cavity is cleaned again with a small brush.

Final result
After about 10-15 minutes the operation is finished and the final result is as shown here.
There are small open wounds, so that the wound fluid can dehydrate up to 6 weeks after the surgery and thus it does not come to a wound infection.
The excision of a pilonidal cyst (sinus pilonidalis)

Excision means cutting out and it means the complete disease in the middle of the buttock. This standard method involves the radical removal of the subcutaneous fatty tissue down to the periosteum. The bone is not affected by the pure skin disease.
In order to be able to assess the extent of the tissue to be removed, the fistula tract used to be filled with a blue dye (methylene blue) and then blue dyed tissue was removed. This sometimes resulted in very radical operations, so that this technique is no longer used in most hospitals today.
The wound is often up to 10cm long and 5cm wide. This is followed by open wound treatment, with daily discharge of wound secretions with a yellowish greasy secretion called fibrin. This is not pus, but a kind of "wound glue", which is very important for wound healing.
The open wound itself cannot usually become infected, as infectious wound secretions can drain off. Only in the case of a congestion of secretions, such as when the wound is closed too early, does infection occur.
In the first 21 days, the wound may additionally hurt and is very sensitive. Small hemorrhages often occur from the wound edge if, for example, the dressing is too tight and is pulled off. These bleedings are annoying but harmless.
During the first 4 weeks, the wound must be rinsed twice a day and after every bowel movement with clear water without soap for about 2 minutes. If this is followed, no foul-smelling wounds will develop. After cleaning, a bandage must always be applied.
Operation time: 5-30 minutes
Hospital stay: 1-2 days, outpatient surgery possible according to findings.
Inability to work: approx. 2-12 weeks
General anesthesia: Usually yes, but also depending on the findings.
Plastic surgeries
For larger findings that are not infected, plastic surgery can be performed instead of extensive excision. The best known methods are the Karydakis operation and the Limberg plastic.
Karydakis operation
We recommend surgery only in case of recurrence. A risk is always a wound infection due to the proximity to the anus , so that in many cases the wound must be opened early after 2-5 days and then heal like an excision.
Outpatient surgery is generally not recommended due to the excessive movement of the patient in the freshly sutured buttock area.
Operation time: 30-60 minutes
Hospital stay: 3-5 days, outpatient surgery is possible according to the findings, but not recommended.
Inability to work: approx. 2-3 weeks
General anesthesia: Usually yes, for smaller findings local anesthesia is also possible.
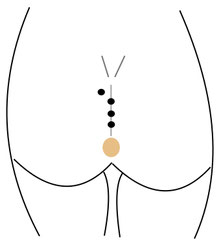
Initial findings
The coccygeal fistula shows here several openings, the so-called pits. One or more of these fistula outlets may also be located laterally. Here, in the upper left corner, is one of these lateral fistula outlets.
If a larger piece of tissue is to be excised with subsequent suturing, plastic surgery according to the Greek surgeon Karydakis is an option.

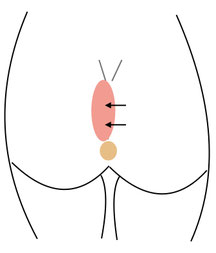
Tissue removal
At the beginning of the operation, which is preferably performed under general anesthesia, the diseased tissue is excised asymmetrically. Here, the defect is shifted mainly to the side with the main defect.
In our example, the main fistula tract is located above on the left side, which is why as much of the left tissue as possible is removed. Complete excision of the fistula tract leaves only healthy tissue for subsequent plastic surgery.
Displacementplasty
After removal of the tissue, the resulting defect must be closed with tissue.
To do this, the surgeon mobilizes the subcutaneous fat tissue on the right side (under the arrows) and pulls all the skin without tension to the left side to resuture the wound edges.

Result
An asymmetrical suture is made, which should not be in the midline if possible, as wound healing is very poor here. A wound drain is inserted, which should remain in place for 2 days.
The sutures are removed after about 12 days. Often the wound is exposed to strong stress even if it is handled carefully, so that wound healing disorders and infections occur quite frequently due to the proximity to the anus.
Limberg operation
This operation is a major plastic surgery with a large wound area. Even with careful handling, the wound is subjected to severe stress, so that wound healing problems and infections often occur due to the proximity to the anus.
When the wound opens, the wound area is very large and the healing time is correspondingly long. Therefore, we recommend this operation only in case of very pronounced findings and then only by plastic surgeons.
Operation time: 60-120 minutes
Hospital stay: 3-5 days, inpatient surgery
Inability to work: approx. 2-4 weeks
General anesthesia: yes
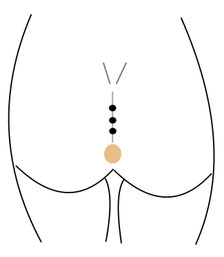
Initial findings
The pilonidal cyst shows here several openings, the so-called pits. One or more of these fistula outlets may also be located laterally.

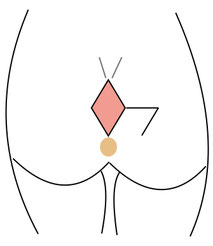
Tissue removal
At the beginning of the operation, which is always performed under general anesthesia, the diseased tissue is excised in a diamond shape.
The complete excision of the fistula tract leaves only healthy tissue for the subsequent plastic surgery.
Displacementplasty
A displacement plastic is prepared to close the defect.
For this purpose, an identical rhombus is drawn in laterally so that this new rhombus can be displaced to the left.

Result
After displacement plastic surgery has been performed, the tissue flap is resewn with several sutures. The sutures in the subcutaneous fatty tissue are self-dissolving, whereas the outer sutures must be removed.
Patients should avoid excessive movement for 3 days, if possible, and the drains are removed after 2 days.